Widening the evidence base for masks
Chapters
0:017:5 Fluid dynamics analysis supports the finding that cloth masks decrease the radius of the droplet cloud
17:30 The impact of droplet cloud radius depends on construction
22:23 WHO's advice uses worst case PPE assumptions, not source control
Transcript
Hi there, my name is Jeremy Howard. I'm a data scientist at the University of San Francisco. I specialize mainly in medical data and recently I had the opportunity to present to a group of, I think entirely or nearly entirely epidemiologists at the World Health Organization who were looking at guidelines for mask wearing and I've had a lot of interest expressed in seeing the slides and the arguments that I put up to the World Health Organization in that so I thought I would share them with you here today.
So I am part of an organization called Masks for All which is a group of volunteers. We're all scientists from many different areas of science, many different parts of the world and we've all spent a lot of time studying the science around community mask wearing and trying to communicate that to the public and to policymakers such as the World Health Organization.
The World Health Organization has recently released some guidelines that have recommended using cloth masks in public or non-medical masks in public and we would actually like to see them go further with their recommendations and make them stronger and change them in some ways but perhaps more importantly one of the things I really focused on was a need to change the kind of evidence that epidemiologists tend to look at for public health interventions like mask wearing, governments and obviously in this case the World Health Organization.
So the WHO actually sponsored a study which was what's called a meta-analysis where it's basically a study of other studies so this is the one here true at L which was published in the Lancet and what we realized is that actually this review which the WHO used quite heavily has a bunch of problems.
The first most obvious ones is that outside of hospitals they only actually looked at three studies so that's what they call non-healthcare settings and in fact two of those studies had major problems. The first is that this one here Lao et al actually is not a study of community or household use of masks at all it was actually a study of the use of masks in hospitals during hospital visits.
And then the second study with a big problem is Tuon et al which actually showed that in this case out of the nine groups that wore masks none of them got sick but it was so underpowered there were so few people in this study that the review used a number here that basically claimed that masks make you more likely to be infected not less likely even though actually nobody got sick who wore a mask in that study.
Basically because there were so few infected people in the study overall it was kind of a statistical aberration as it were. So the only one which really studied community mask use was this one Wu et al which actually the number they used includes families where some people weren't wearing masks.
So if you just actually include the ones where they were there was a only there was basically a 70% reduction in risk in the households that used masks. The study also looked at mask use in hospitals and this is the table that they included but actually only three of the studies in this case were of COVID-19 and in fact I should mention none of the studies in non-healthcare were of COVID-19 they were all of SARS 1.
And the three healthcare studies of COVID-19 actually showed over 95% decrease in risk amongst those using masks in healthcare but they basically did the statistical analysis in a very strange way maybe not strange very common way but not really appropriate for this which is that they assumed that SARS, MERS and COVID-19 all had the same profile in terms of what do masks do and as a result they gave these three studies really low weights 0.9%, 0.9% and 1.7%.
So even though the risk reduction from using masks for COVID-19 in all three cases was was huge those studies were basically ignored in this meta-analysis. There is one analysis actually of wearing masks in households for COVID-19 which is this one here and in this case there was a about an 80% reduction in risk in the households that wore masks so that's that's good you know it's a it's a pretty strong study it's not huge you know it's it we would love to see a bigger version of it but it's a it's a start.
The problem is though that for all of these kinds of studies they're very hard to interpret because you know when you're trying to say what's the impact of wearing a mask on transmission if I wear a mask my hope is that I'm you know if I'm sick and I don't know it that I won't pass on that sickness to other people.
So how do you know if me wearing a mask stopped other people from getting sick? You don't really right because people who come across me wearing my mask will have come across lots of other people as well so if they do get sick was it because a sickness got through my mask or was it because they came in contact with somebody else who was sick?
Who knows right so the only way to study that properly really would be to actually have like 50 cities where everybody in those cities were told not to wear masks and 50 cities where everybody was told they have to wear masks and then get compliance to work and then compare them and that would be basically logistically and ethically impossible.
So in fact the epidemiology and evidence-based healthcare communities have started to realize it well I shouldn't say started to actually for decades have realized this but have particularly been talking about this as being an issue for COVID-19 which is that population health interventions like tell everybody to wear a mask end up being implemented as natural experiments and their evaluation is more complex than a randomized controlled trial that's just the way it is you know we can't hope to find an RCT a randomized controlled trial for a public health intervention like this because it's just not ethical or logistically possible to do.
So that was in BMG Journal of Epidemiology and Community Health in Pillow West Medicine Trish Greenhouse said something similar upstream preventative public health interventions aimed at supporting widespread and sustained behavior change across the whole population like masks rarely lend themselves to a controlled on versus off intervention design randomized controlled trial style design.
So the reason I pointed this out to the World Health Organization was to kind of say look these are the kinds of studies that most epidemiologists are used to studying that you all want to study but they're just not going to happen for this right and so you actually have to look at a wider field of evidence.
So this is what we did we being this group of 19 scientists including epidemiologists and biostatisticians and aerosol scientists and sociologists lots of different folks we all got together to study the evidence across a much wider evidence base than just traditional epidemiological evidence and so we ended up with I think 155 references might even be more now and that became the most viewed paper ever of any kind on preprints.org.
And you know one of the things we looked at in this paper is that we now have a lot of these natural experiments which is that over 80% of the world now lives in regions that require masks. Furthermore in countries like for example in the US over 70% of the population has to wear masks in the US because of state or city specific mandates but back in early to mid-March only 10 countries required masks.
So this change means that we can actually look at kind of the before versus after effects of what happens when countries bring in or when in the case of the US for example states bring in mask requirements. So a paper from Loeffler et al looked at nearly 200 countries and you have to be very careful right because often when people bring in a mask mandate a country brings in a mask mandate they'll do a bunch of other things at around the same time they might have a lockdown at around that time they might have school closures at around that time.
So statisticians have to use multivariate analysis to try to account for these confounders which Loeffler's paper for example did they looked at 10 different policy health interventions all the ones tracked by Oxford across as well as lots of demographic geographic and so forth confounders as well. And they found that countries that did not wear masks when you look at kind of the number of days since the start of the infection or the outbreak in that country after a couple of months that we had huge outbreaks normalized per million population countries where masks were required within 15 days of the initial infection had basically no infection at all and those that required them in the first 16 to 30 days had a bit of an outbreak but they quickly got it under control.
So this is a super interesting data obviously and we see something very similar in a paper by Lewin Waby which is this one here which is that mask mandates in the US very similar result are associated with a 2 percentage point decrease in COVID-19 growth rate 2 percentage points a day that's enormous after 21 days after signing.
So they guessed that by late May somewhere around 200 to 400,000 cases had been averted. So these are often called ecological studies and they're super unpopular amongst many in the epidemiological community there's this idea of this thing called the ecological fallacy which many people misinterpret as meaning you can't generate any understanding of population behavior or the underlying individual behavior of those populations by looking at population data.
But actually data scientists and statisticians and machine learning folks have actually been studying exactly that for many, many decades and in fact there's another paper called the fallacy of the ecological fallacy which is to say basically the ecological fallacy is this kind of grab bag of multiple different issues which for which there are ways to deal with them.
So we should be very careful not to throw away these vitally important studies it's vitally important information because it's really the only kind of data direct data that we can get about the impact of these population health interventions. We can however get lab data and in some ways this is kind of the strongest and most obvious because you can actually literally see here's an example of somebody speaking and this researcher when they're speaking you can see that little tiny droplets come flying out of their mouth and thanks to the use of this laser scattering chamber we can actually see them.
Normally you can't they're too small to see these can be around 10 microns in size in terms of what's visualized here and you can see here they're holding a paper towel over their face just a normal paper towel and when they do almost all of the droplets are blocked it looks like there's two got through.
Now of course you can see he's holding it quite carefully here which obviously if you're using a paper towel or a cloth mask you want it to be as nicely tightly fitting as possible but the basic idea is that yeah you know as you would expect a physical barrier blocks this physical thing which is the droplets that transmit the virus so we can very directly see the way a mask does in fact stop this vector of transmission this key vector of transmission.
So why do we focus on speech droplets? Well the reason we focus on speech droplets is this is a respiratory infection so how does this respiratory infection get transmitted through stuff coming out of your mouth and nose. One way for that to happen is sneezes and we really haven't looked at sneezes much because that is a symptom and so people who are symptomatic hopefully are staying home.
Another is breathing but breathing is mainly going to bring up drop very tiny droplets from your lower respiratory tract which actually it turns out is something where the disease kind of appears later on again after you have symptoms. So what we mainly care about is the upper respiratory tract viral shedding and this comes out in speech droplets so this is why we're particularly interested in speech droplets because these are the ones that people who are walking around don't even know they're sick are rejecting from their mouth.
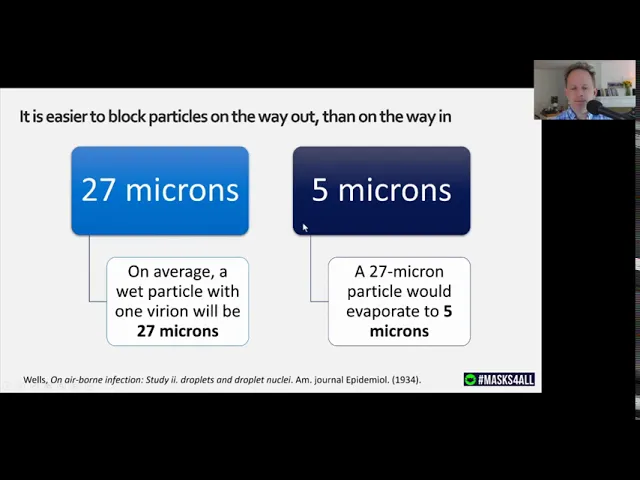
So one of the key things to realize this is not just for speech droplets but particularly so is that on average a wet particle with one variant will be about 27 microns across which is pretty giant compared to the size of the virus but what happens is after it comes out of your mouth it rapidly evaporates down to in this case it would be down to about 5 microns in size.
There's a whole range of droplet sizes but the key is that they will evaporate and become smaller and so when they come out of your mouth they're moving straight forward straight into the fabric they're pretty big the atmosphere inside your mask is very humid because of your breathing and so it hits then this large droplet hits the fabric of your mask and soaks into it so it doesn't go through and then once it becomes much smaller after evaporation if you're not wearing a mask it can float in the air and as it does so it now also doesn't have that direct trajectory so it's also much easier for it to squeeze through the gaps above or around your mask so it's much easier to do what's called source control which is blocking it on the way out and this is why we focus on this idea my mask protects you your mask protects me.
Now some aerosol some tiny droplets maybe from breathing are also important in transmission we don't really know for sure we suspect maybe not so much for the folks that don't have symptoms yet but even if the breathing droplets are important as well we actually know from a study that the basic cloth masks are actually about the most effective at stopping both the the direct coming through the front and through coming out the sides breath because cloth masks can often be like larger cover more of the face and there also can be more absorbent so you know we shouldn't assume that cloth masks are less effective than other masks or most importantly we shouldn't assume that they're not effective at all the lab data we have suggests they are and also remember that most of those countries that now require masks which covers the vast majority of the world's population aren't using medical masks because they're not available so the results we're seeing in practice are from people who are largely wearing simple unfitted masks.
So how long does that droplet cloud stay in the air for well this study showed that when you again look at this laser scattering chamber and you look at the speech droplets that come out they after coming out of the mouth at minute zero after about 10 minutes about half of them have fallen to the ground and after 20 minutes maybe three quarters have but you can see there's still a large droplet cloud even 20 minutes after somebody speaks so these droplets if they're not blocked on the way out they can actually hang around for quite a long time.
A fluid dynamics study found something pretty similar about the effect of masks which is that if you don't wear a mask your droplet cloud can go out beyond two meters where else with a mask it really is well contained you can see with a mask a little bit of it goes backwards but the actual radius of the cloud is much smaller.
So how much is this impact of the size of the rejection in size of the droplet cloud so a study in physics of fluids found that the amount of reduction in size of the droplet cloud depends a lot on what kind of mask you're wearing all kinds of mask at least made it at least half the radius but a stitched mask with cotton was the most effective in terms of getting it down to just 2.5 inches in this study.
So one of the interesting things is that since a mask can make the droplet cloud smaller that means that social distancing becomes more helpful becomes more important because you're not as likely to infect somebody six feet away. Another reason that there's a great impact on social distancing is that a study found that people who didn't wear masks people tended to stay closer to them than people who did wear masks.
So in other words when you see somebody wearing a mask there's this conscious or unconscious thing going on where people actually keep their distance away from you more. I guess maybe it's this like reminder of like oh this is a pandemic there's somebody in a mask you know I should I should keep her a healthy distance.
So that's interesting because some folks have claimed including the WHO that wearing a mask could reduce to less could result in less social distancing but the data we have doesn't support that at all it seems populations that wear masks have dramatically less transmission it seems that the effect on social distancing is much better because of the reduced droplet cloud size and that people may even keep their distance more.
In terms of children which is particularly important right now schools seem like a particularly important place to wear masks it's it's somewhere where people talk a lot and so therefore a lot of speech droplets in places like Sweden where they didn't close the schools kids had just as high an infection rate in in seroprevalence studies as adults did so it seems like when you don't close schools kids become infected often and then they go on to pass on those infections to adults even though the kids themselves rarely get seriously sick it seems that they just as often or maybe nearly just as often pass on that sickness to adults and so for example in Victoria the largest outbreak in the whole state came from a school in Israel there was massive outbreaks around the country both Victoria and Israel are both places where COVID-19 was almost under control and they reopened schools and things got totally out of control and in fact you know it when you look at the viral loads in kids they tend to be pretty similar to the viral loads in in adults.
So one of the things that we talked about is is this idea of likely harms the World Health Organization currently has a list of likely harms under the section around community mask use. So some of the likely harms that we've heard about a lot and seen in the World Health Organization's guidelines don't really seem likely at all in fact some of them seem like likely benefits rather than likely harms and for example there's a claim that there could be a increased risk of self-contamination but actually it's much more likely you would see a decreased risk a mouth covers the mouth and nose making it much harder to touch them and so there has been some studies of this it does need more research but the evidence we have suggests that maybe this is a benefit rather than a harm.
There's also a claim in the guidelines that there's a risk of droplet transmission and it splashes to the eyes which is true of course but that is not the result of mask wearing that's just like oh also guys cover up our eyes. So it's kind of strange to me that there are these that you know official health bodies like the WHO include these likely harms when they're not likely or harms necessarily or related to wearing a mask it's it's really odd to I don't really know what's going on here.
There's a claim often including the WHO guidelines that there could be a likely to be a false sensor security but there's actually no data supporting that and in fact it was claimed over a hundred years ago and it's never been demonstrated. So this is just this kind of speculative well maybe it might happen.
So I think we've got to be very careful of when you see somebody saying here are some likely harms is to say like do we have any evidence of that is there any data to support that is there any lab evidence of that or is this just an assertion which somebody's just made up and could could the opposite be equally true.
The other issue with the WHO guidelines is that it it lists some suggested types or a particular type of mask based on a table of mask filtration levels and actually the the advice is based on studies which don't use the right kind of approach. In particular they look at particle sizes of 72 nanometers.
Now that's very very small very small and much smaller than the five microns we talked about and in fact it's it's very hard to even come up with a droplet smaller than one micron that can both hold together you know at all and actually contain a very on a virus particle.
So the particle size that's being studied but in the WHO table is way smaller than we would expect to ever need to filter in practice particularly for source control. So when it's coming out as we discussed it's larger than when it's coming in. So you know that's a much smaller particle than we actually think you should be looking at.
Furthermore they used a flow rate so the amount of particle you know the amount of gas going through the machine that they were testing with was was much higher than you would have in real life when you're kind of sitting or walking slowly or something like this. So in fact the the particle sizes and flow rates they used are based on the testing criteria for masks as protective equipment for health care workers which is like worst case situation not really that appropriate for for community use.
Also they didn't actually test the best materials and so there there are actually tests of materials that that you can buy from Amazon or the local shop or whatever which are orders of magnitude more effective than the ones that that they talked about and even recommended in their guidelines.
So I think it's a waste that they're not actually pointing out that there are much better materials available. They also didn't touch on the best designs for ensuring a good fit. Again I think that's a real shame for example this rubber mask brace or this approach I'm wearing here of just three rubber bands were shown to surpass the N95 fit test so the kind of health care medical worker fit test in in most situations that this study looked at.
So there are a lot of crafters now working with you know great materials and great designs for example on Etsy if you look for face masks with a moldable nose wire and an insertable filter where you can put these really great filter materials there's over 69,000 different shops where you can buy these from kind of DIY crafters.
So you know we I think it's good it would be great if public health bodies can try and provide this information about what are the best approaches and and realize that they are available. Okay so that's it for my little summary of what we talked about and what I presented to the World Health Organization on community mask wearing and I hope you found that helpful.
Thanks for watching.